Use the link below to listen to this week's episode. Subscribe to Med On The Go on Podbean, iTunes, and Google Play so that you'll never miss an episode.
https://medonthego.podbean.com/e/med-on-the-go-episode-19-informed-consent-and-informed-discharge/
Running diagnostics

Wednesday, February 28, 2018
Consent (as applicable in Canada)
As usual, this blog post is available in podcast form. Look for Med On The Go on Podbean (www.medonthego.podbean.com) , iTunes, and Google Play. If you haven't already done so, check out our Facebook page at www.facebook.com/drolimedonthego. If you would like to support us, please visit www.patron.podbean.com/medonthego for more details.
Medico-legal issues are such “downers” to talk about, but in
this day and age it really needs to be discussed because we all want outcomes
that are safe and fair for all parties involved. Since I’m hoping to practice
medicine in a different country than the one I was trained in, it’s especially
important for me to learn about the laws and regulations in Canada.
According the Canadian Medical Protective Association (CMPA)
three criteria required for informed consent:
1.
Patient must have the mental capacity to
understand the nature and possible consequences of the procedure/treatment.
2.
The patient must be fully informed about the
procedure/treatment.
a.
The physician should disclose the diagnosis.
b.
The physician should disclose the nature of the
proposed investigation/treatment.
c.
The physician should disclose the expected
consequences for forgoing the proposed investigation/treatment.
d.
The physician should disclose reasonable
alternatives to the proposed investigation/treatment.
e.
The physician should disclose any material risks
of the proposed investigation/treatment and answer questions posed by the
patient.
i. Not
every possible complication needs to be conveyed to the patient.
ii. Complications
that occur frequently should be disclosed.
iii. Complications,
however rare, with significant consequences for the patient (e.g. death,
paralysis) need to be disclosed.
iv. Risks
that a reasonable person in the patient’s position would consider significant
should also be disclosed.
3.
The consent must be given voluntarily
The consent form itself does not equal real consent. The
explanation given by the physician and the dialogue between physician and
patient about the proposed procedure/treatment is the all-important element of
the consent process (no explanatory pamphlet/video can replace this, but if
supplementary material was provided it should also be documented). A signed
form will be of relatively little value later if the patient can convince a
court that the explanations were inadequate or absent. A summary of the consent
discussion entered into the medical record at the time is the best defense
against an allegation of lack of informed consent; the documentation of the
consent discussion need not be lengthy or detailed. The physician can delegate
the responsibility of obtaining consent to a colleague, medical trainee, or
nurse who has the knowledge and experience to provide information tailored to
the requirements of the patient and circumstances.
In witnessing a signature, the witness simply confirms the
identity of the patient who signed the document and that the person’s mental
state at the time appeared to allow for an understanding of what was signed.
The witness has no obligation to provide pre-treatment explanations and is in
no way attesting to the adequacy of the explanations given by the physician.
If a surgeon at a teaching hospital delegates certain
surgical procedures to his/her trainees, he should disclose to patients the
involvement of trainees in these procedures.
Battery in the medico-legal context is when a physician
carries out an investigation/treatment in the absence of valid consent or when
treatment went beyond or deviated significantly from that for which consent was
given. Assault and battery may also apply when consent was obtained by way of
serious misrepresentation.
In the emergency department, however, consent is not needed
when a patient is at imminent risk of serious injury AND obtaining consent is
either not possible or would increase risk to the patient. This rule assumes
that most people would want to be saved in an emergency. However, a capable and
informed patient can refuse treatment or part of treatment (even if it is
life-saving); and emergency treatment CANNOT be initiated if a competent
patient has previously refused the same or similar treatment (for same problem)
and there’s no evidence to suggest he has changed his mind or an advanced
directive (such as DNR) is available. Refusal of help in a suicide situation
still warrants treatment. When in doubt, initiate treatment; it can be
withdrawn at a later time.
Children presenting to the ER are treated in the same way:
treat immediately if the patient is at imminent risk. The patient does NOT have
to reach age of majority to give a valid informed consent. However, if the
patient in question is obviously not capable to make a decision (like a baby or
toddler), parents/guardians have the right to make treatment decisions; if they
refuse treatment that is life-saving or will potentially alter the child’s
quality of life, Children’s Aid Society (CAS—there is one in every hospital)
must be contacted, in which case the consent of CAS is needed to treat.
Common issues needing consent include HIV testing and
administration of blood products. Jehovah’s Witnesses are the most common group
who will have issues with latter; they may refuse all blood products (even
autologous), in which case treatment needs to provide the highest possible
quality of care with out the use of blood products (e.g. crystalloids for
volume expansion like hydroxyethyl starch). They will generally sign hospital
forms releasing medical staff from liability.
An extension of informed consent is the topic of informed
discharge. During informed consent, patients are informed of what can
potentially go wrong; during informed discharge, patients are informed of the
symptoms and signs that would indicate something wrong may be happening. They
should also be given a sense of urgency of the response required and where best
to seek medical attention. The information should be tailored to each patient
and clinical situation.
In the emergency room setting, for many patients there are
diagnostic uncertainty on an initial/subsequent visits. These patients should
be made aware of this uncertainty—what is known and what is unknown—so that any
continuation, escalation, or change in symptoms may prompt reevaluation. Just
like informed consent, a discussion between physician and patient is warranted;
any detailed explanatory pamphlet or video would not suffice. Documentation of
the advice provided on discharge should be documented in the medical records.
Thursday, February 22, 2018
Med On The Go episode 18
For those of you who prefer to listen than read...
Subscribe to our podcast on Podbean, iTunes, and Google Play!
https://medonthego.podbean.com/e/med-on-the-go-episode-18-altered-level-of-consciousness/
Subscribe to our podcast on Podbean, iTunes, and Google Play!
https://medonthego.podbean.com/e/med-on-the-go-episode-18-altered-level-of-consciousness/
Altered Level Of Consciousness
Today's post is also available in podcast form; visit www.medonthego.podbean.com to stream or download!
If you haven't already done so, also check out our Facebook page www.facebook.com/drolimedonthego --it has some hilarious medicine-related jokes and some useful, applicable articles too. If you wish to support us, please see www.patron.podbean.com/medonthego for more details!
Altered mental status is a collective, non-specific term
referring to change in cognitive function, behavior, or attentiveness. It
includes delirium, dementia, lethargy (state of decreased awareness and alertness
i.e. patient may appear wakeful), stupor (unresponsive but rousable), and coma
(sleep-like state, not rousable to consciousness).
Possible causes of coma (AEIOU TIPS)
Acidosis/alcohol
Epilepsy
Infection
Oxygen (hypoxia)/opiates
Uremia
Temperature/trauma (esp. to head)
Insulin (too little or too much)
Psychogenic/poisoning
Stroke


Remember “GCS < 8 intubate!” Ability to protect airway is
first priority.
History
·
Obtain collateral from family, friends, police,
paramedics, old charts, or Medic Alert bracelets etc.
·
Onset and progression
o Antecedent
trauma, seizure activity, fever
o Abrupt
onset suggests CNS hemorrhage/ischemia or cardiac cause
o Progression
over hours to days suggests progressive CNS lesion or toxic/metabolic cause
·
Determine patient’s baseline level of
consciousness
·
Past medical history, paying attention to
similar episodes, overdose, or concurrent psychiatric disorders (e.g.
depression).
Physical examination
·
Vital signs including temperature
·
Cardiac, respiratory, and abdominal exams
·
Complete neurological exam
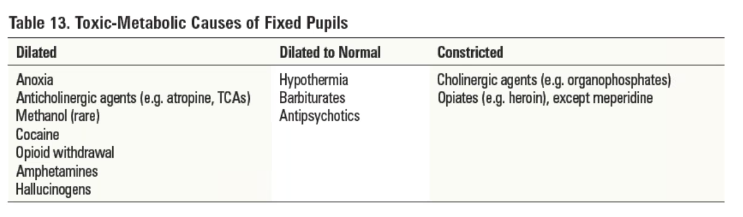
o Pupil
size and reactivity
o GCS
Investigations
·
Blood work—rapid blood sugar, CBC, electrolytes,
creatinine, BUN, liver function test, glucose, serum osmolality, venous blood
gas, coagulation studies, troponins
·
Imaging—CXR, CT head
·
Other tests—ECG, urine analysis, urine
toxicology
Diagnosis
·
Administer appropriate universal antidotes
o Thiamine
100mg IV if history of alcoholism or patient looks malnourished
o One
ampule D50W IV if low blood sugar
o Naloxone
0.4~2mg IV or IM if opiate overdose is suspected
·
Distinguish between structural and
toxic-metabolic coma
o Structural
coma
§
Pupils, extra-ocular movements, and motor
findings are usually asymmetrical
§
Look for focal or lateralizing abnormalities
o Toxic-metabolic
coma
§
Dysfunction at lower levels of the brainstem
(e.g. caloric unresponsiveness)
§
Respiratory depression in association with an
intact upper brainstem (e.g. equal reactive pupils)
§
Extra-ocular movements and motor findings are
symmetrical or absent
·
Essential to re-examine frequently because
status can change rapidly
·
Diagnosis may become apparent only with the
passage of time. Delayed deficit after head trauma suggestive of epidural
hematoma (characteristic “lucid interval”).
Disposition
·
Admission if ongoing decreased level of consciousness
·
Discharge if altered level of consciousness is
readily reversible; ensure adequate follow-up care
Friday, February 9, 2018
Genitourinary Tract Injuries
Welcome back to Med On The Go! This week we discuss genitourinary tract injuries commonly seen in the emergency room setting. Before we start, I'd like to invite you to visit our Facebook page www.facebook.com/drolimedonthego/ and help us by pressing "like". As usual, this blog post is also available in podcast form; subscribe to Med On The Go With Dr. Oli on iTunes, Google Play, or Podbean to make sure you never miss an episode. If you'd like to further support us, please visit www.patron.podbean.com/medonthego for more details.
Now let's dive into this week's topic:
Genitourinary tract injury secondary to trauma can occur any where within the genitourinary tract by
a variety of mechanisms.
·
Blunt trauma—often associated with pelvic
fractures
o Upper
tract
§
Renal
·
Contusions (minor injury—parenchymal ecchymoses
with intact renal capsule)
·
Parenchymal tears/lacerations—non-communicating
(hematoma), communicating (urine extravasation, hematuria)
§
Ureter: rare, at uretero-pelvic junction
o Lower
tract
§
Bladder—gross hematuria usually suggests bladder
injury
·
Extraperitoneal rupture of bladder from pelvic
fracture fragments
·
Intraperitoneal rupture of bladder from trauma
and full bladder
§
Urethra
·
Posterior urethral injuries: MVCs, falls, pelvic
fractures
·
Anterior urethral injuries: blunt trauma to
perineum, straddle injuries/direct strike
o External
genitalia
·
Penetrating trauma—damage to kidney, bladder,
ureter (rare), external genitalia
·
Acceleration/deceleration injury—renal pedicle
injury—high mortality rate (laceration and thrombosis of renal artery, renal
vein, and their branches).
·
Iatrogenic injury—ureter and urethra damage
secondary to instrumentation
History
·
Mechanism of injury
·
Hematuria (microscopic or gross), any blood on
underwear
·
Dysuria, urinary retention
·
History of hypotension
Physical examination
·
Abdominal pain, flank pain, CVA tenderness,
upper quadrant mass, perineal lacerations
·
DRE: sphincter tone, position of prostate,
presence of blood
·
Scrotum: ecchymoses, lacerations, testicular
disruption, hematomas
·
Bimanual exam, speculum exam
·
Extraperitoneal bladder rupture: pelvic
instability, suprapubic tenderness of mass of urine or extravasated blood
·
Intraperitoneal bladder rupture: acute abdomen
·
Urethral injury: perineal ecchymosis, scrotal
hematoma, blood at penile meatus, high riding prostate, pelvic fractures
Investigations—in gross hematuria, the GU system is
investigated from distal to proximal (i.e. urethrogram, cystogram… etc.)
·
Urethra: retrograde urethrography
·
Bladder: urinary analysis, CT scan, urethrogram
+/- retrograde cystoscopy +/- cystogram (distended bladder and post-voiding)
·
Ureter: retrograde ureterogram
·
Renal: CT scan (best, if hemodynamically
stable), intravenous pyelogram
Management
·
Urology consultation
·
Renal injury
o Minor
injuries—conservative management such as bed rest, hydration, analgesia,
antibiotics
o Major
injuries—admit
§
Conservative management with frequent
reassessments, serial urine analysis +/- re-imaging
§
Surgical repair (exploration, nephrectomy) for
hemodynamically unstable patients or those who continue to bleed > 48hrs,
major urine extravasation, renal pedicle injury, all penetrating wounds and
major lacerations, infections, renal artery thrombosis
·
Ureter injury—ureterouretostomy
·
Bladder injury
o Extraperitoneal
§
Minor rupture—Foley drainage for 10~14 days
§
Major rupture—surgical repair
o Intraperitoneal—drain
abdomen and surgical repair
·
Urethral injury
o Anterior—conservative
treatment, consider Foley catheter or suprapubic cystostomy and antibiotics for
those who cannot void
o Posterior—suprapubic
cystostomy (AVOID CATHERIZATION) +/- surgical repair
Subscribe to:
Comments (Atom)
Upper GI Bleeds
As always, this blog post is available in podcast form at www.medonthego.podbean.com. You can also find Med On The Go on iTunes and Google ...

-
ER series 3 — Heat stroke In the previous week we’ve been experiencing crazy good weather in Vancouver—so good that when I took a frien...
-
 As always, this blog post is available in podcast form at www.medonthego.podbean.com. You can also find Med On The Go on iTunes and Google ...
As always, this blog post is available in podcast form at www.medonthego.podbean.com. You can also find Med On The Go on iTunes and Google ... -
As usual, this blog post is available in podcast form. Look for Med On The Go on Podbean (www.medonthego.podbean.com) , iTunes, and Google P...