
Today's post is also available in podcast form; visit www.medonthego.podbean.com to stream or download!
If you haven't already done so, also check out our Facebook page www.facebook.com/drolimedonthego --it has some hilarious medicine-related jokes and some useful, applicable articles too. If you wish to support us, please see www.patron.podbean.com/medonthego for more details!
Altered mental status is a collective, non-specific term
referring to change in cognitive function, behavior, or attentiveness. It
includes delirium, dementia, lethargy (state of decreased awareness and alertness
i.e. patient may appear wakeful), stupor (unresponsive but rousable), and coma
(sleep-like state, not rousable to consciousness).
Possible causes of coma (AEIOU TIPS)
Acidosis/alcohol
Epilepsy
Infection
Oxygen (hypoxia)/opiates
Uremia
Temperature/trauma (esp. to head)
Insulin (too little or too much)
Psychogenic/poisoning
Stroke


Remember “GCS < 8 intubate!” Ability to protect airway is
first priority.
History
·
Obtain collateral from family, friends, police,
paramedics, old charts, or Medic Alert bracelets etc.
·
Onset and progression
o Antecedent
trauma, seizure activity, fever
o Abrupt
onset suggests CNS hemorrhage/ischemia or cardiac cause
o Progression
over hours to days suggests progressive CNS lesion or toxic/metabolic cause
·
Determine patient’s baseline level of
consciousness
·
Past medical history, paying attention to
similar episodes, overdose, or concurrent psychiatric disorders (e.g.
depression).
Physical examination
·
Vital signs including temperature
·
Cardiac, respiratory, and abdominal exams
·
Complete neurological exam
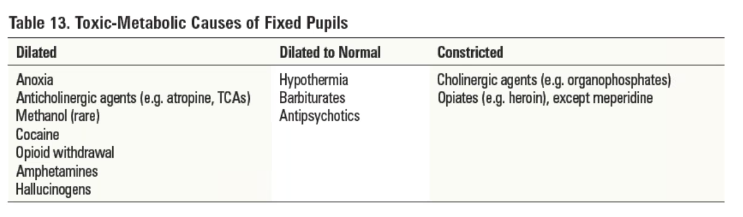
o Pupil
size and reactivity
o GCS
Investigations
·
Blood work—rapid blood sugar, CBC, electrolytes,
creatinine, BUN, liver function test, glucose, serum osmolality, venous blood
gas, coagulation studies, troponins
·
Imaging—CXR, CT head
·
Other tests—ECG, urine analysis, urine
toxicology
Diagnosis
·
Administer appropriate universal antidotes
o Thiamine
100mg IV if history of alcoholism or patient looks malnourished
o One
ampule D50W IV if low blood sugar
o Naloxone
0.4~2mg IV or IM if opiate overdose is suspected
·
Distinguish between structural and
toxic-metabolic coma
o Structural
coma
§
Pupils, extra-ocular movements, and motor
findings are usually asymmetrical
§
Look for focal or lateralizing abnormalities
o Toxic-metabolic
coma
§
Dysfunction at lower levels of the brainstem
(e.g. caloric unresponsiveness)
§
Respiratory depression in association with an
intact upper brainstem (e.g. equal reactive pupils)
§
Extra-ocular movements and motor findings are
symmetrical or absent
·
Essential to re-examine frequently because
status can change rapidly
·
Diagnosis may become apparent only with the
passage of time. Delayed deficit after head trauma suggestive of epidural
hematoma (characteristic “lucid interval”).
Disposition
·
Admission if ongoing decreased level of consciousness
·
Discharge if altered level of consciousness is
readily reversible; ensure adequate follow-up care


No comments:
Post a Comment